One of the collections held by the Arthur H. Aufses, Jr. MD Archives is the Roosevelt Hospital School of Nursing records (1896-1974). A gift to the collection is a scrapbook from alumna Evelyn I.V. Howard, class of 1908, who captured images of her fellow classmates and house staff physicians during her years in training there. Included among her friends were images of Nina Gage, who went on to join a missionary outreach in Changsha, Hunan Province in China in 1909. Gage worked in the hospital created by the team, and established a nursing school for both men and women. The scrapbook includes images of the hospital founded by the team as well as the nursing school students’ classes and hospital scenes sent to Howard by Gage. They illustrate an important time in the development of China’s medical history.
This is the cover of the Howard scrapbook, which is wrapped in the blue and white striped cloth of the Roosevelt Hospital School of Nursing student uniform. The Roosevelt family coat of arms and motto is pictured at the bottom right. The Roosevelt family coat of arms, as depicted here in blue and black, includes a rosebud bearing three roses with a crest consisting of a helmet and three ostrich plumes. The family motto in the ribbon below the crest reads “Qui plantavit curabit” which means “The one who planted it will take care of it” or “He who will plant will cultivate.”
NURSING IN CHINA
Nursing, as a profession, was almost unheard of in pre-20th century China. Traditional Chinese healers diagnosed patients by observing various parts of the body – the tongue, the pulse (taken in both arms), and asking extensive questions. They then prescribed herbal remedies, massage, acupuncture or other methods to balance yin and yang – the two great opposing and complimentary forces in nature – to bring the body back into balance. (Forgive the simplification; this is a very basic explanation of Chinese medicine.) The family themselves, or their servants, in wealthy households, treated the patient at home – hospitals were also introduced by western missionaries – following the prescribed treatment. It is significant to note that most of the care givers were men.
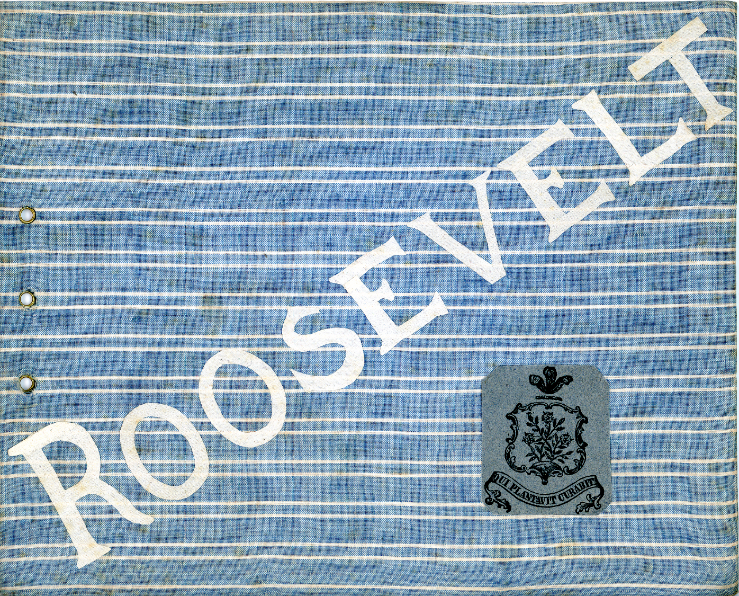
Bathing a hospital patient
Men’s medical ward decorated for Christmas. The man in black is a probationer (nursing student in training).
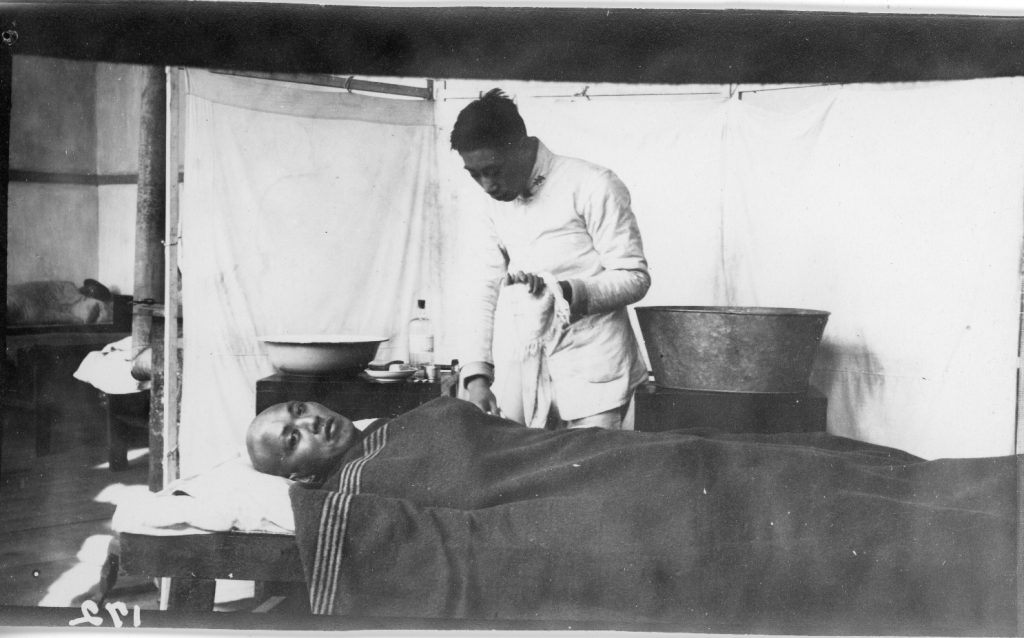
Feeding a helpless patient in Yali Hospital.
THE YALE-IN-CHINA MISSION
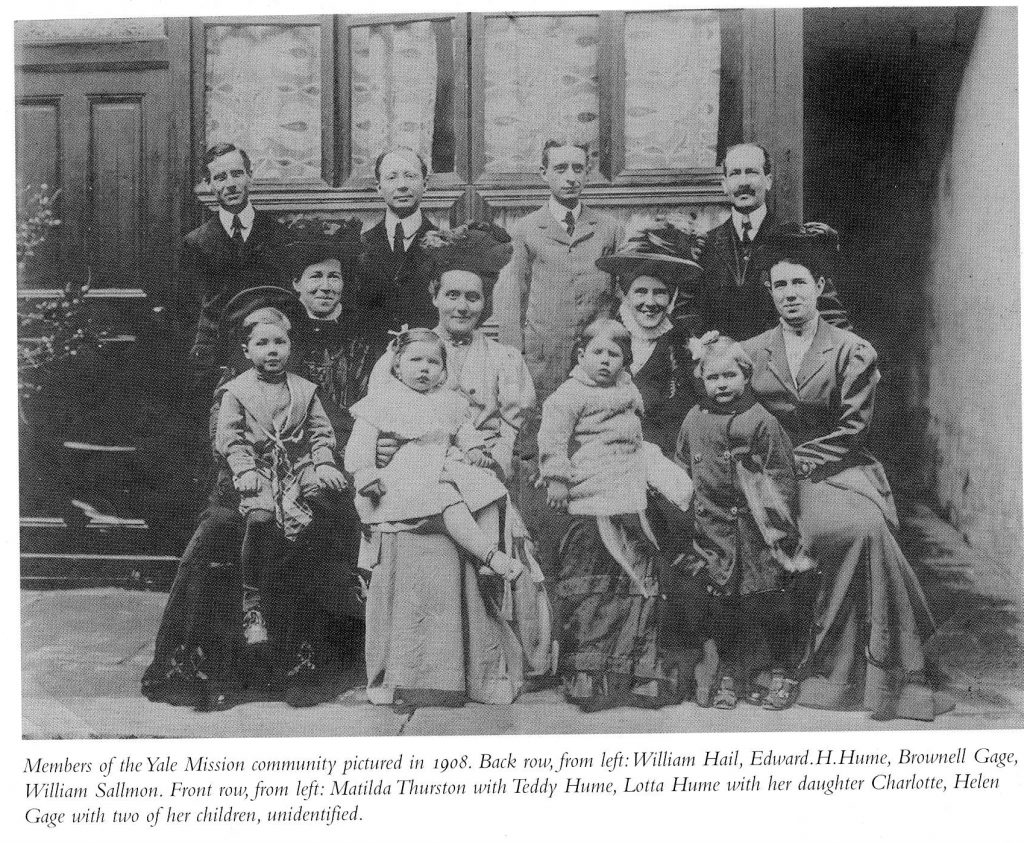
Starting in the 1880s, western missionaries brought modern medical methods to various large cities of China where they established missions’ projects. One team, organized by Yale University’s Christian Missions Society, was the Yale-in-China mission. The team consisted of members of the Yale class of 1898 and their families. Additionally, Nina Gage, a 1908 graduate of the Roosevelt Hospital School of Nursing, and sister to team-member Brownall Gage, joined them in 1909 to work as a nurse in the hospital/clinic and to help establish a modern nursing program.
One of the team members, working with experienced missionaries from a northern project, arrived in 1902 to visit possible cities to establish the work. He then reported back to the Yale Missions Society board and the project team about the cities he visited for their consideration. Eventually they chose the city of Changsha, Hunan Province in southern China to establish the Yale-in-China Mission. Selected for its large size, Changsha was considered extremely clean and well built, according to the more experienced missionaries. Changsha’s alleys were paved with granite and it had a good sewage system, compared to other cities. Other missionaries had high opinions of the people there, citing them as born leaders who were very independent and influential in Chinese culture and life.
Map of southern China, highlighting Hunan province and the city of Changsha (this image and the following two are courtesy of Nancy E. Chapman)
In 1904, the team rented two buildings near the center of the city that were large enough to support their plans to establish a prep school and college, a medical school and hospital/clinic, as well as a nurse training school. One building was large enough to carve out several classrooms and dormitory space for students and housing for the team, while the other building served as a hospital/clinic.
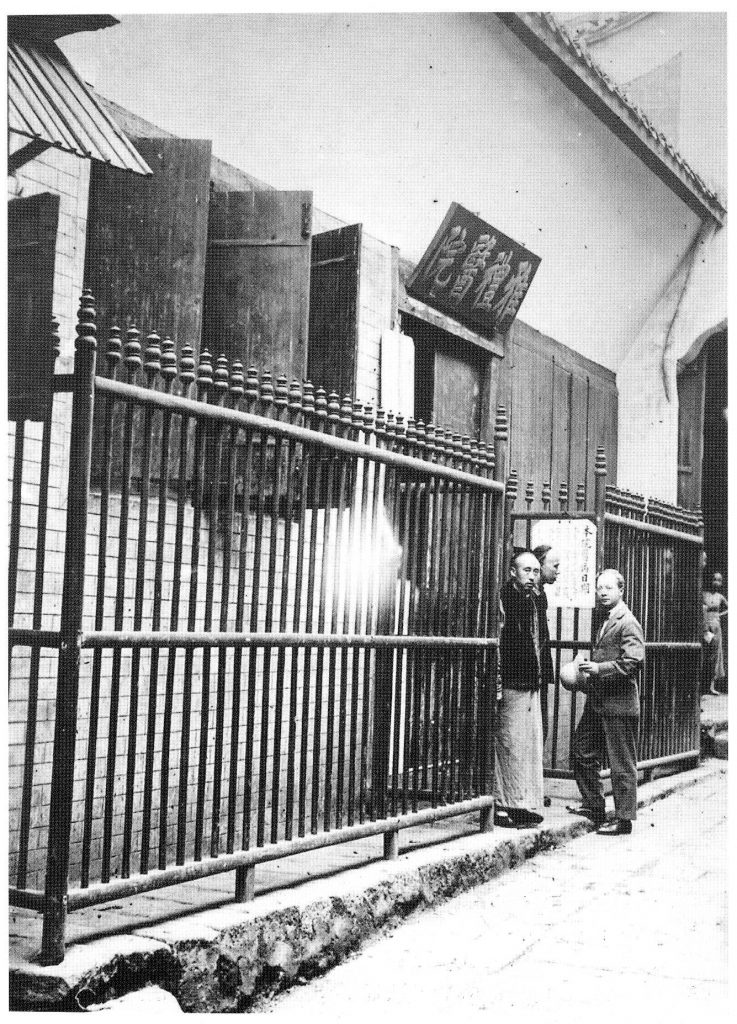
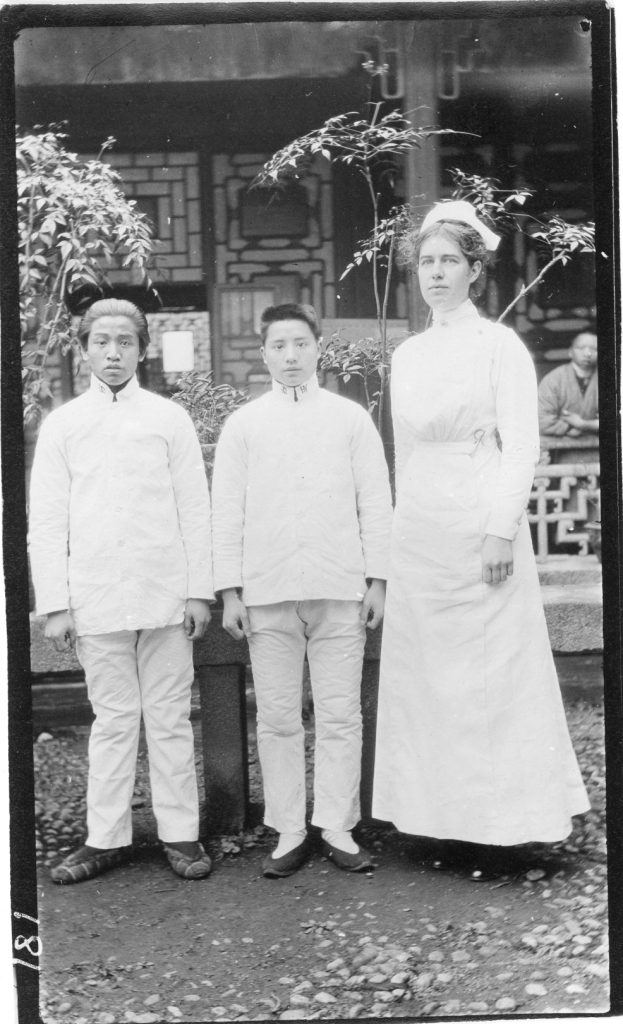
Left: The Yale Mission’s early medical work was led by Edward Hume, M.D., Yale class of 1897. Hume (right) is pictured with two Chinese colleagues at the door of the mission’s first clinic and hospital, housed in a converted inn in the crowded center of Changsha.
NINA D. GAGE
Nina Diadamia Gage was born in 1883 in Brooklyn, and she and her siblings grew up in and around New York City. She attended Wellesley College, where, like her older brother, she was an active member of the missionary committee. After graduating, Gage entered Roosevelt Hospital’s Training School for Nursing, which had opened in 1896. (Roosevelt Hospital was renamed Mount Sinai West in 2015.)
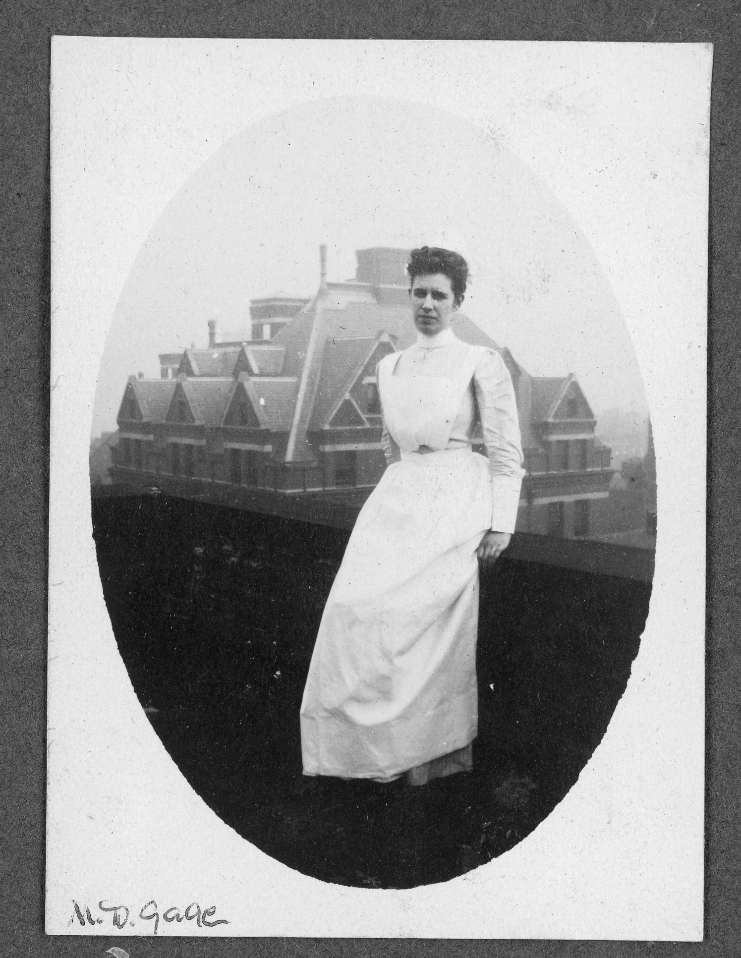
Nina Gage as a student nurse, relaxing on a building rooftop, at Roosevelt Hospital’s School of Nursing, circa 1907
At that time, student nurses were trained at the bedside by the senior student nurses, as graduate professional nurses were few in those years. The junior nurses, who served as floor staff, were taught to take vitals, change bandages, feed and clean patients, note changes in the patient’s condition to report to the attending physician during rounds, and keep the ward itself clean. Weekly lectures by the staff physicians supplemented and expanded the bedside training. Monthly lectures considered a different area of medical care. One would assume these lessons were repeated by Gage to her Chinese students.
After graduating in 1908, Gage was employed as a night nurse while making the necessary arrangements to move to Changsha in 1909 to join her brother and the Yale team. She thought it was important to learn the language, and took that first year to study it while she worked in the “Yali Hospital” (as it was called) clinic and assisted the doctors in surgery and planning the establishment of the nursing school, which opened in 1913.
This image captures nurse Gage in preparations for surgery at the Yali Hospital, undated (note: faded original image)
THE HSIANG-YA NURSING SCHOOL
Since nursing as a profession was new in China, Gage had the interesting – and daunting – privilege to create the Chinese name for it. She selected “Scholars to Watch and Guard” or more briefly, “Guard Scholars” – to indicate nurses.
Advertising posters were hung around the city to announce the opening of the school, inviting “both boys and girls to be admitted for training in a new profession” (Hume, E., p. 168). The entrance requirements for the “Scholars to Watch and Guard” training were two years of middle school and passing the school’s entrance examinations in Chinese and arithmetic. Parental consent and the payment of school fees were also required. On examination day, twenty girls and forty boys arrived to take the tests. A few applicants backed out, intimidated by the exam questions, but in the end, five girls and seven boys became the first class of trainees.
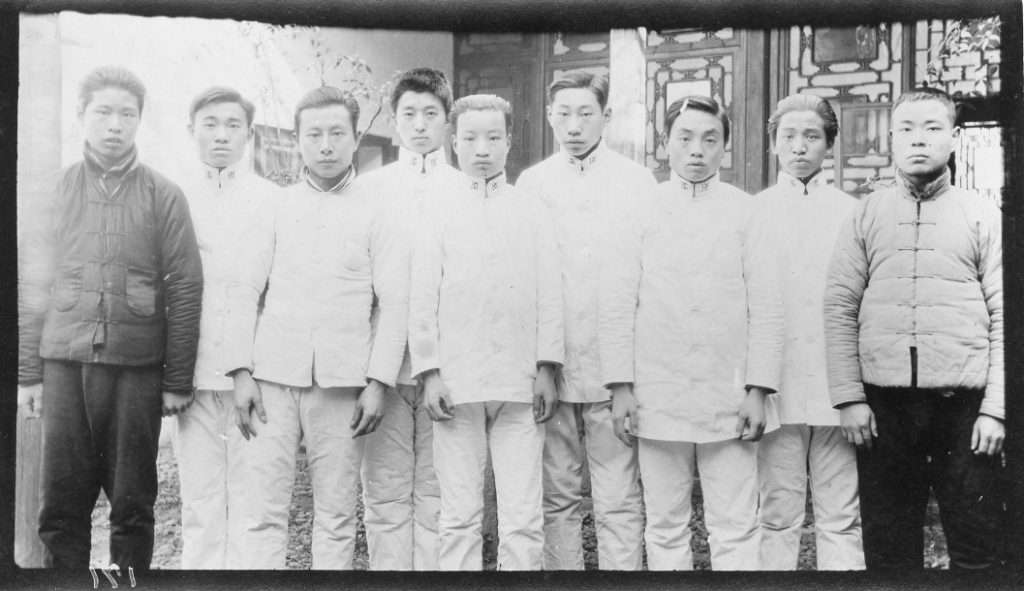
Nurses and probationary students in the Men’s Nursing School division, undated
Female students, in particular, had problems gaining entrance, as at that time, girls were prepared from a young age for marriage and lived very secluded lives, neither meeting nor socializing with boys outside of immediate family. However, once they demonstrated success in passing the entrance exams, doubtful parents were content to allow them to continue and in the end were very proud to have graduate ‘Guard Scholar’ daughters in crisp white uniforms, ready to serve their communities in such a positive way.
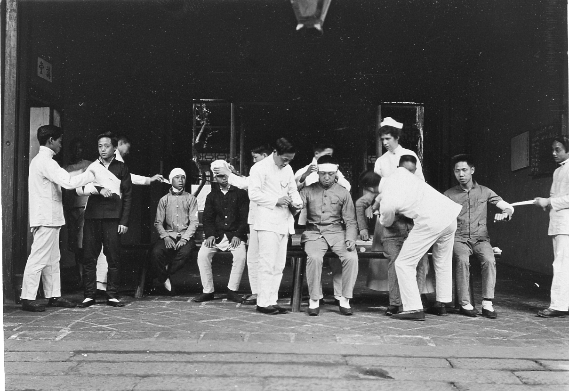
The images above and below are of bandaging class practice. Men and women were taught separately, out of respect for Chinese culture, which kept women apart from men who were outside of their immediate family. Likewise, only men worked in the men’s ward and the women in the women’s wards, at least until the 1930s, by which time women dominated the nursing field in China.
Initially the nursing school and hospital were simply called the Yali School, but in the early teens, both were renamed “Hsiang-Ya” – “Hsiang” indicating “Hunan” and “Ya” indicating “Yale,” highlighting the partnership of Hunanese teachers and students with the Yale teachers and administrators.
Yale School front courtyard, 1909 (note: faded original image)
Preparing salt solutions, 1915
Preparing and sorting of supplies, 1915
In 1927, due to the on-going political turmoil, all foreigners were expelled from China, the Yale-in-China Mission closed, and the team returned to the United States. By 1929, however, the Yale-in-China work resumed, but under Chinese leadership and direction. The hospital and schools of the Yale Mission continue to exist to this day, though they have been absorbed into larger university settings. The relationship between Yale University and China also continues to this day as Yale-China (雅礼协会), based in New Haven, CT, which “bridges the United States and China through collaborative partnerships in education, healthcare, and the arts” (The Yale-China mission statement, from their webpage).
Most of the photographs in Ms. Howard’s scrapbook have short captions on the back, usually with dates. This one reads: “During the Tuchun’s war – bringing in wounded,” unfortunately it is undated.
Gage is among the handful of notable women who brought modern professional nursing to China. In additional to teaching and working in the hospital, Gage helped found the Nurses’ Association of China (NAC) in 1909, signifying the start of a professional nursing movement in the country. The founding members were mostly western missionary nurses who came together to organize, but they were soon joined by Chinese colleagues. By 1915, China established an examination system for the professional certification of nurses, followed by other advances to promote nursing education across the Asian continent.
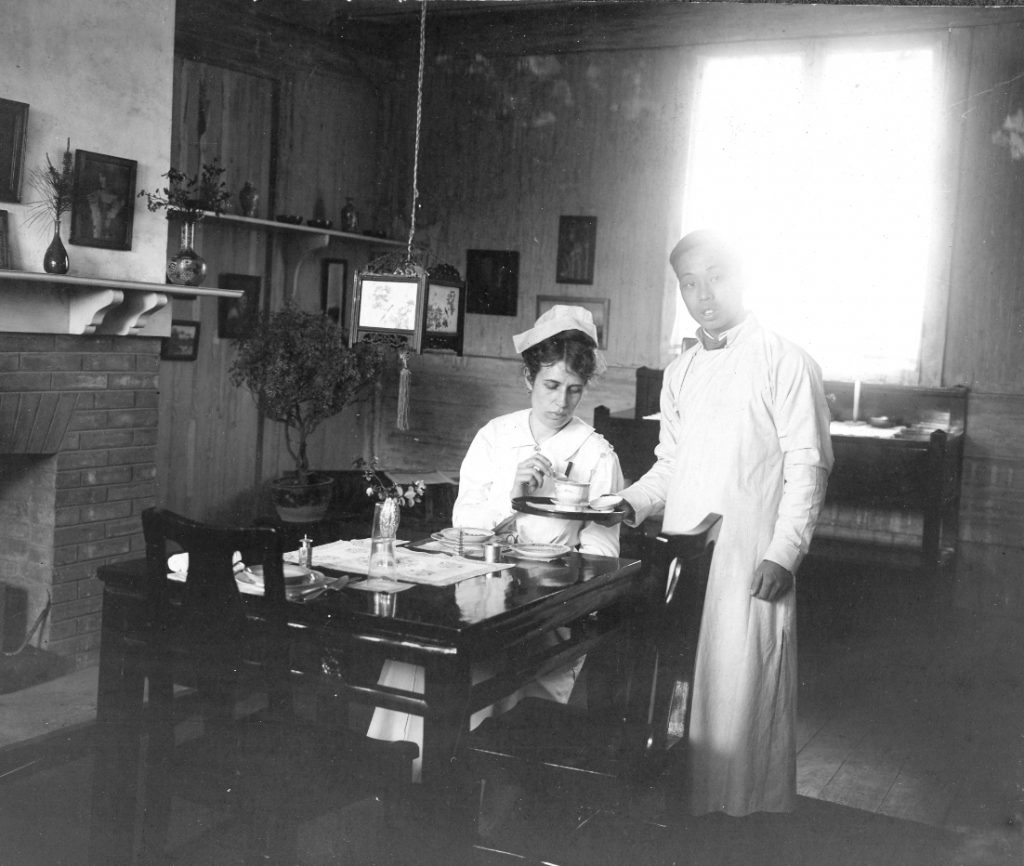
Nina Gage taking a meal in her home, circa 1915
In 1912, Gage was elected as the first president of the NAC, serving a two-year term. She went on to serve as the chairperson of its education committee. After a brief return to the U.S. during WWI, where she taught wartime nursing at Vassar, Gage returned to Chine and was appointed Dean of the Hsiang-Ya Nursing School, as it was renamed.
Superintendent Gage and the senior class of 1915
GAGE’S POST-CHINA LIFE
Upon returning to the United States in 1927, Nina Gage continued to work in nursing and was active in its support organizations. From 1925 to 1929, she served as president of the International Council of Nurses, representing China. She was executive secretary of the National League for Nursing Education from 1928 to 1931. In 1930, during her term as president of the Roosevelt Hospital School of Nursing Alumnae Association, she started The Roosevelt Hospital School of Nursing Alumnae Association Bulletin, later renamed The Roosevelt Review, which published news about alumnae activities but also included articles on developments in nursing practice and medicine in general. Throughout her working years, Gage remained active in the National Nursing Association and the American Nurses Association. Gage also published several articles on nursing in China for The American Journal of Nursing and as well as authoring two books: A General History of Nursing in 1933 and Communicable Diseases in 1940.
In the U.S. Gage continued working as a teacher to the next generation of professionals. In 1927 she became educational director and director of the nursing department of the Willard Parker Hospital in NYC. In 1931, the historically Black Hampton Institute (Hampton, VA) appointed Gage as director of its new nursing school. She taught at the Jersey City Medical Center Nursing School during the 1934-1935 school year and then went to the Newport Hospital (Newport, R.I.) as director of its school of nursing from 1935 to 1943. In 1949, Newport Hospital’s Gage Hall was named in her honor. From 1943 until her retirement in 1945, she was the Director of Nursing at the Protestant Hospital in Nashville, Tennessee. She died on October 18, 1946, at the age of 63.
Yuhong, Jiang. “Shaping modern nursing development in China before 1949.” International Journal of Nursing Science. 2016 Dec 29; 4 (1): 19-23. https://pubmed.ncbi.nlm.nih.gov/31406712/
Dr. Frank B. Berry, pictured above, was born in Dorchester, Mass., in 1892. He attended Harvard College (Class of 1914) and Harvard Medical School, graduating in 1917. His medical training was interrupted by World War I, in which he served as an Army pathologist with the American Expeditionary Forces in France.
When he returned home, he interned at Peter Bent Brigham Hospital and at Boston City Hospital, initially completing a residency in pathology. However, Berry developed an interest in surgery during the war. He chose to take an internship at Presbyterian Hospital (NYC), and a surgical residency at Bellevue Hospital (NYC), where he continued to practice as the director of its first Surgical and Chest Surgical Division under Columbia University’s College of Physicians and Surgeons section.
In 1936, Dr. Berry was appointed to Roosevelt Hospital as an Associate Attending Surgeon in thoracic surgery. At the start of World War II, Roosevelt Hospital was asked to form the Ninth Evacuation Hospital with hospital staff, and Berry was appointed Chief of Surgery of the unit. The “Ninth Evac” was one of the earliest units ashore in the North African landing and the unit was far forward during the Tunisian campaign. The unit traveled extensively through Northern Africa, Sicily, Italy, France, and Germany before returning home.
Dr. Berry also served as consultant in surgery at Allied Forces Headquarters. In 1944, he accompanied the Seventh Army during its invasion of Southern France and through the campaign to Augsburg, Germany. At the end of the war, Berry accepted the post of Deputy Chief of Public Health and Welfare of the Allied Control Commission in Germany, tasked with reopening German medical schools. He resigned as Associate Attending Surgeon (thoracic) at Roosevelt Hospital in 1946, and was appointed Visiting Consultant in general surgery (thoracic). He remained in the Army Reserves, becoming a brigadier general in 1949 and played a prominent part in furthering the reserve program in New York City’s Military District.
Berry began to experience tremors in his hands in the early 1950s, and decided it was prudent to move on from surgery. Between 1954 and 1961, he held the position of Assistant Secretary of Defense focusing on health and medical affairs. During this time, he developed what came to be known as the Berry Plan. The plan allowed medical students to avoid being “called up” arbitrarily, say in the middle of their schooling or in-hospital training, throwing a wrench into school enrollment plans, hospital staffing plans, and the education of many medical students. Applicants could request one of three schemes: to complete an internship year and then go in the service, to complete one year of residency then go into the service, or serve after completing full residency training. Each of these choices would then involve two years of active duty military service, and in some cases, additional reserve service years. Doctors didn’t always get the option they applied for, but they were able to complete some part of their training without interruption and were guaranteed a spot to continue where they left off once they returned from service; 42,000 physicians and surgeons took advantage of the Berry Plan, including many of our own MSHS physicians and surgeons.
Writing about Dr. Berry as a person, a former resident at Roosevelt Hospital, Edward G. Stanley-Brown says that he devoted enormous amounts of time and energy in teaching each one of the trainees. He took a personal interest in their lives, often acknowledging personal and professional events and successes with a note or phone call. His door was always open to his house staff. He was happy to assist a new intern with a simple procedure or work with a senior resident on the most complicated one. He could be stern and demanding in surgery, requiring residents to be courteous, pleasant and to arrive at the OR on time, or be dismissed for that session, but his reprimands were firm, fair and carried out in private. Stanley-Brown remembers him fondly as “a superb surgeon, a brilliant teacher … a true friend, and quite simply our beloved chief.”
Frank Berry died on October 14, 1976 at the age of eighty-four. His funeral took place in St. Bartholomew’s Church four days later. Stanley-Brown notes that it must have been a bad day to need a surgeon in NYC, because the church was full of them. Surgeons from Bellevue, Roosevelt, St. Luke’s, Presbyterian Hospitals and other sites, including every one of his intern group, came to honor the man who made such a difference in the education and lives of thousands of physicians and surgeons across the country.
Written by Michala Biondi, Associate Archivist
Sources: Stanley-Brown, Edward G. “Frank Brown Berry, 1892-1976,” Bulletin of the New York Academy of Medicine, Vol. 54, #5, May 1978, pp. 532-538. Berry, Frank B. “The Story of ‘The Berry Plan.’“ Bulletin of the New York Academy of Medicine, Vol. 52, #3, Mar/April 1976, pp. 278-282. Clark, Alfred E. “Frank B. Berry, Chief of Defense Doctors,” New York Times, October 16, 1976 Greene, Frederick L. “Remembering the Berry Plan.” General Surgery News, May 15, 2020 Wikipedia, “The Berry Plan.” https://en.wikipedia.org/wiki/Berry_Plan retrieved March 1, 2023
James Henry Roosevelt, whose bequest founded the Roosevelt Hospital, was born at his family’s home on Warren Street, NY, NY on November 10, 1800. Following his earlier education in neighborhood schools, he enrolled in Columbia College, where his studies included law, and was graduated from there in 1819. He subsequently set up a law practice in New York City.
With his studies behind him, and his law practice established, he stood on the threshold of a promising life. Described as a young man of pleasing appearance, brown hair, above-average height and with a gentle and courteous demeanor, he was well-to-do, brilliant, and engaged to be married to Julia Boardman, who was from an old New York City family.
However, a sudden illness that left him physically disabled, ending his plans for both career and marriage. The exact nature of the illness is unclear: Some speculated that it was lead poisoning from a home remedy for a cold, concocted of hot milk into which lead shot had been boiled. Others think he fell victim to poliomyelitis.
In any case, largely incapacitated, he abandoned his law practice. Not wanting to ‘burden’ Julia Boardman with his disability, he broke his engagement to her. (Neither married and both remained lifelong friends; in fact, one of the few bequests he made, outside of the one to his nephew, James C. Roosevelt Brown, and the monies left to found The Roosevelt Hospital, was an annuity for Ms. Boardman, whom he also named as executrix of his will.)
Roosevelt then embarked on a life not just of physical limitations, but also of frugality and austerity, devoting much of his time and interests to real estate dealings and to the management of his securities; he thus increased his worth substantially. It is thought that he conserved and increased his funds for one specific purpose: to support “the establishment in the City of New York of an [sic] hospital for the reception and relief of sick and diseased persons.” Whatever the reason, when he died on November 30, 1863, he left almost one million dollars toward that objective.
The hospital founded under the terms of his will was to be a voluntary hospital that cared for individuals regardless of their ability to pay. It seems reasonable to suppose that having himself suffered from illness, he realized the plight of those who might at the same time be afflicted with both sickness and destitution. We celebrate its 151st anniversary of its opening on November 2nd.
It is said that Roosevelt was never morose or gloomy. He maintained an active interest in the life about him and in the affairs in which he could not participate. He enjoyed the companionship of a host of friends, one of the closest being Julia Boardman.
Although James H. Roosevelt’s remains were first buried in his family’s vault in the New York City Marble Cemetery, they were moved to the Roosevelt Hospital grounds when a monument to him was placed there in 1876. In late 1994 the monument was removed and relocated and his remains were exhumed. In the spring of 1995 Roosevelt was re-interred in the New York City Marble Cemetery family vault. Julia Boardman’s remains were interred in the same cemetery, but in her father’s vault.
Since the 2013 merger of the Continuum Health Partners into the Mount Sinai Health System, medical students working in the System’s hospitals have earned their MDs from the Icahn School of Medicine at Mount Sinai. Newer staff and students may be unaware that prior to 2013, the Continuum Health Partners, made up of St. Luke’s-Roosevelt Hospital, Beth Israel Medical Center and the New York Eye and Ear Infirmary, now all a part of Mount Sinai’s System, played host to medical students attached to a different medical school. In fact, from very early days, Roosevelt Hospital and her sister institution, St. Luke’s Hospital, were associated with Columbia University’s College of Physicians and Surgeons (P&S), though Roosevelt’s ties are closer. How did this come to be exactly?
In 1885, P&S was located on East 23rd Street and Fourth Avenue, now known as Park Avenue South. William H. Vanderbilt, an American businessman and philanthropist, died in December of that year. He left a legacy of $300K and a plot of land on West 59th Street between Ninth and Tenth Avenues to P&S for the express purpose of building a new medical school, the largest donation to a medical school up to that time.
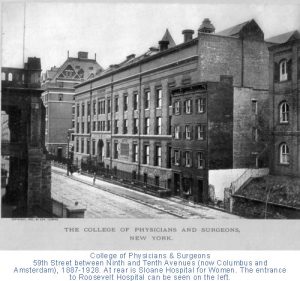
The College of Physicians and Surgeons on West 59th Street across from Roosevelt Hospital. You can see the Hospital’s Administrative Building port-cohere front column to the left in the image. (Photo source: Archives & Special Collections, Columbia University Irving Medical Center.
It just so happened that the Roosevelt Hospital, which had opened its doors several years earlier, was across the street from the new building. Of the twelve physicians chosen to be the first clinical staff of the Hospital, almost all of them were P&S alumni and held teaching positions there. It probably was no surprise to the staff to see medical students from P&S coming over to observe their professors’ clinics and surgeries.
By 1914, P&S students received bedside teaching on patient wards; by 1936, fourth-year students were allowed into the operating rooms. In 1928, the College of Physicians and Surgeons moved to the newly constructed medical center campus at 168 Street in Washington Heights, but their students continued to travel to clinical training at Roosevelt, and a number of other hospitals in the area.
Surprisingly, in over sixty years of P&S student training at Roosevelt Hospital, there was only a ‘handshake’ agreement between the medical school and the Hospital. However, by the late 1940s, there was discussion on the subject, and on October 24, 1951, the Board of Trustees put into place a formal affiliation with Columbia University’s College of Physicians and Surgeons, allowing the students of the medical school to work at the hospital as part of their formal training. The agreement was signed by all parties on May 12, 1952. In 1971 it was renewed and expanded.
Medical studies aren’t the only tie between Columbia and Roosevelt Hospital, however. In 1964, an affiliation agreement between Columbia University’s School of Dental and Oral Surgery and Roosevelt Hospital was signed allowing dental students in to the surgery. That same year a two-year program in anesthesiology for the registered nurses was established at Roosevelt to help end the shortage of practitioners in this area. This program moved to Columbia University’s School of Nursing after the Roosevelt Hospital’s School of Nursing closed, and the loose ends of Roosevelt’s program merged with Columbia’s. The CRNA program – Certified Registered Nurse Anesthetists – continues there to this day.
With the 2013 merger of St. Luke’s-Roosevelt Hospital Center into the Mount Sinai Health System, ties to Columbia University’s programs may have come undone, but the history and influence of each institution upon the other remains, in the drive to produce outstanding medical professionals.
Nurses’ Week has come and gone, but it is always worthwhile to celebrate our healthcare warriors and shine a light on their accomplishments. This post would like to highlight Elise Galloway, a 1906 graduate of the Roosevelt Hospital School of Nursing who went on to be a Roosevelt nurse for her whole career.
Elise Galloway
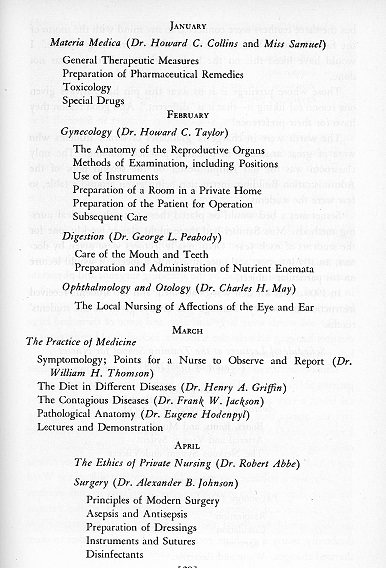
Galloway was born in Garrison, New York in 1878. The farmhouse she and her family lived in until the 1920s still stands on the property of the Garrison Grist Mill Historic District site. As a student, she would have worked one of two shifts – 7a.m. to 7p.m. or the reverse – 7p.m. to 7a.m. Nursing students generally had one half day off a week, two hourly breaks a day and time on Sundays for church. The bulk of their training would be on their assigned ward. Their responsibilities included daily grooming and washing of patients’ faces, hands and feet, weekly sponge bathing, taking temperatures and noting that and any other particular changes in the patients’ condition, changing dressings, and serving patients their meals and preparing additional special dishes, if a patient needed supplemental nourishment. Nurses would join the Attending Physician on rounds, noting instructions and assisting as needed. Student nurses would also have weekly lectures in anatomy, physiology, Materia Medica, gynecology, the digestive system, the practice of medicine, the ethics of private nursing, and surgical diseases and emergencies.
RHSON Class of 1906 – I believe she is sitting below Miss Samuels who is in the back row, fifth woman in from the left.
Galloway graduated with the class of 1906, and began working at Roosevelt right out of school. Miss Mary Alexander Samuels, was the exacting Directress of Nursing in charge of both the nursing staff and the nursing school. Miss Samuels, considered a keen observer, recognized Galloway’s fine nursing skills, and heard about her reputation for reliability and an ability to catch on quickly – a necessary skill for a job that was learned by doing. She assigned Galloway as nurse supervisor over the Syms Operating Theatre.
The Syms Theatre, opened in 1892, was one of the most advanced operating theaters in the country and had very high standards. Medical students from the College of Physicians and Surgeons, located across the street from the Hospital, trained there, and visiting surgeons frequently came to observe surgical procedures in its sky-lighted amphitheater. As Nurse Supervisor, Galloway had to make sure all her student nurses knew how to properly sterilize instruments, suture materials, towels, and sheets for surgery, something that was a long and complex process at that time, as well as how to work with the surgeons during a procedure. Galloway, noted as being a patient and kind teacher, earned the nickname, “Mother Galloway,” used by students and doctors alike.
Her Hospital service was interrupted only twice in her career – the first time was in 1915, for six months, while Galloway volunteered to work in France with the American Ambulance Corps, prior to the formal U.S. entry into World War I. When the U.S. joined the conflict, Galloway served as a member of Base Hospital 15, which was composed of doctors, nurses, and support staff all drawn from Roosevelt Hospital’s personnel. She served as the Nursing Supervisor, organizing the operating room staff much as she did in the Syms Theatre.
Officers and Nurses of Base Hospital 15. Elise Galloway is on the left, standing next to the Unit Head wearing the Mountie-type hat.
The unit remained in Chaumont, France for most of the war. However, Galloway, along with another nurse and, two doctors spent about ten weeks at a French evacuation hospital at the French front near Vasney, where she experienced air raids at close range in exchange for valuable experience in wound treatment techniques.
Returning home to the Syms Theatre and New York, doctors knew her as an invaluable assistant and friend; nurses knew her as an excellent teacher. She was said to have an unfailing good temper, always calm, retaining poise in any emergency, and very unselfish, presenting the profession of nursing nobly and exemplifying the spirit of service and high standards that nursing is strives for.
The alumni newsletter notes that Elise Galloway left Roosevelt Hospital after an operation in the summer of 1933, and died in the Hospital on September 20, 1934 after an illness of several months.