Aug 3, 2021
On August 27th, it will be 165 years since the first baby was born at The Mount Sinai Hospital in 1856. The mother was a Mrs. Lichtenstein. She named the baby Isaac Touro, in honor of a Hospital benefactor, Judah Touro (1775-1854), who had helped support the young Jews’ Hospital in New York, as Mount Sinai was then known. (Judah Touro also gave money for the founding of Touro Infirmary in New Orleans and today’s Touro College and University System is named for Judah and his father Isaac.)
Isaac Touro Lichtenstein was one of two babies born in the Hospital during its first year of operation. Until the 1920s, most babies were born at home or in one of the specialized women and child care hospitals around the City. This meant that many general hospitals, including Mount Sinai, never felt the need to add a formal obstetrical service to their offerings, thus limiting the number of babies born at the hospital over the years.
By the 1920s, as hospital births began to rise around the country, the Mount Sinai medical staff started to talk to the Board of Trustees about adding obstetrics. As the doctors saw it, the problems arising from not having babies born at the Hospital were: the Gynecology staff could not admit their obstetrical patients to Mount Sinai; there was no obstetrical training for the GYN residents, nor was there training for the pediatrics residents in newborn care. The last also applied to The Mount Sinai Hospital School of Nursing, which affiliated with the Sloane Hospital for Women so students could fill the gap in their education.
While the Trustees were increasingly sympathetic with the request to add an obstetrical service, it wasn’t until the middle of the 1940s that concrete plans were made for the erection of a new building to house obstetrics and gynecology, today’s Klingenstein Pavilion on Fifth Avenue. Every new building demands a fundraising campaign to make it a reality. Mount Sinai had just finished a major expansion that ended in 1922, with the addition of a new School of Nursing building and a semi-private pavilion seen as the next priorities. When these two buildings opened, the Depression was in full swing, which sapped Hospital and potential donor resources. This was followed quickly by World War II, but by the mid-1940s, the Hospital could see a window of opportunity on the horizon.
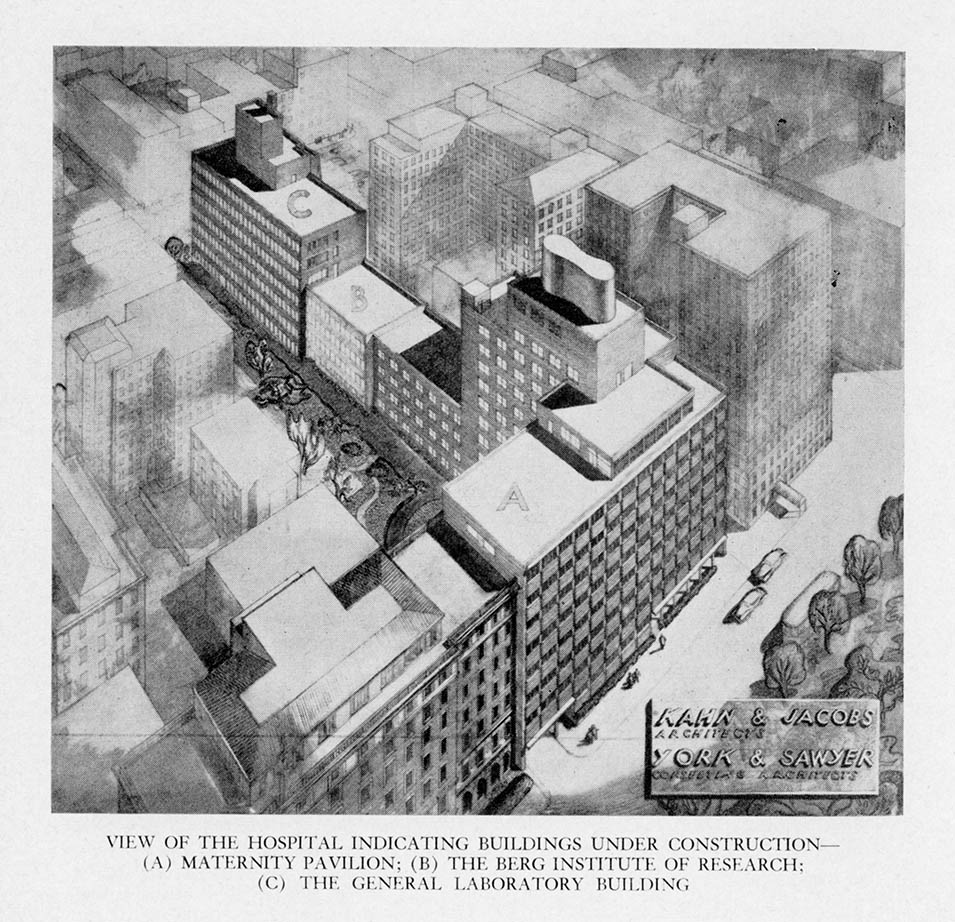
A fundraising campaign was begun when the war ended and on July 22, 1948, ground was broken for three buildings: the Klingenstein Pavilion, and the Atran and Berg Laboratories. In 1952, the obstetrical service started to operate as the building slowly opened. July marked the start of Mount Sinai’s first Prenatal Clinic, and the first prenatal clinic for women with diabetes in New York City started in the fall. The first OB patients were admitted in October, with the first baby born October 29, 1952 – 96 years after Isaac Touro Lichtenstein.
Jun 21, 2021
I recently spent some time reviewing the President’s Report section of the Annual Report of The Mount Sinai Hospital from 1921 (linked here, starting on page 190). The President then was George Blumenthal, a devoted trustee, and a smart businessman who had recently guided the Hospital through a major expansion program, the uncertainties of World War I, and the influenza epidemic of 1918. Reading the report reminded me of the joys – and problems – with reading primary historical sources: it is very easy in hindsight to see connections between two times that may not be related, and simple observations can seem very prescient.
Don’t get me wrong, parts of the report are very dated and irrelevant to today: the Hospital was unable to afford radium to use in patient treatment, and so that service was not provided. There was also a section on issues related to fund raising through the Federation of Jewish Charities (today’s UJA-Federation). But still, there were many issues that would seem familiar to our current leaders. The Hospital was perennially short of money, but after the epidemic and the war, wages were rising quickly for what today would be called “essential workers”. Adding to this was a restrictive immigration policy that limited the labor pool. The inability to hire as many trained nurses as they needed was a continuing struggle as well, something the whole country recognizes today.
George Blumenthal, President of The Mount Sinai Hospital from 1911-1938
And yet Blumenthal made the case – as we do today – for why private hospitals like Mount Sinai deserve the philanthropic support of the people. He says:
It is absolutely essential that private institutions like Mount Sinai should be leaders of progress in hospital work…. To discover, test and demonstrate new methods of treatment is recognized as one of the functions of private institutions and it is one of the strongest reasons for their existence and constitutes their most important claim on the generosity of the public which supports them.
A couple of pages later, Blumenthal makes a bold statement about the importance of Mount Sinai being a teaching hospital. At this time it had loose clinical ties to both Columbia and NYU. He envisioned something more:
A Hospital possessing the clinical and laboratory resources of Mount Sinai should have university affiliation or if this be impracticable should independently utilize its organization for teaching purposes, for in no other way can the fullest benefits be derived from the intensive study of interesting, varied and often perplexing clinical material. We hope the day is not very far off when work on these lines can be done either through affiliation with one of the many teaching institutions located in our city or by independent action.
And “independent action” it was. Even with academic affiliations with various medical schools, in the 1950s Mount Sinai was not satisfied that they were living up to their potential in terms of training the next generation of physician/scientists or using their immense clinical material for creating new medical knowledge to advance patient care. In 1963, the Trustees received a charter to create their own medical and graduate schools. The Mount Sinai School of Medicine opened in 1968.
Jun 9, 2021
Nurses’ Week has come and gone, but it is always worthwhile to celebrate our healthcare warriors and shine a light on their accomplishments. This post would like to highlight Elise Galloway, a 1906 graduate of the Roosevelt Hospital School of Nursing who went on to be a Roosevelt nurse for her whole career.

Elise Galloway
Galloway was born in Garrison, New York in 1878. The farmhouse she and her family lived in until the 1920s still stands on the property of the Garrison Grist Mill Historic District site. As a student, she would have worked one of two shifts – 7a.m. to 7p.m. or the reverse – 7p.m. to 7a.m. Nursing students generally had one half day off a week, two hourly breaks a day and time on Sundays for church. The bulk of their training would be on their assigned ward. Their responsibilities included daily grooming and washing of patients’ faces, hands and feet, weekly sponge bathing, taking temperatures and noting that and any other particular changes in the patients’ condition, changing dressings, and serving patients their meals and preparing additional special dishes, if a patient needed supplemental nourishment. Nurses would join the Attending Physician on rounds, noting instructions and assisting as needed. Student nurses would also have weekly lectures in anatomy, physiology, Materia Medica, gynecology, the digestive system, the practice of medicine, the ethics of private nursing, and surgical diseases and emergencies.

RHSON Class of 1906 – I believe she is sitting below Miss Samuels who is in the back row, fifth woman in from the left.
Galloway graduated with the class of 1906, and began working at Roosevelt right out of school. Miss Mary Alexander Samuels, was the exacting Directress of Nursing in charge of both the nursing staff and the nursing school. Miss Samuels, considered a keen observer, recognized Galloway’s fine nursing skills, and heard about her reputation for reliability and an ability to catch on quickly – a necessary skill for a job that was learned by doing. She assigned Galloway as nurse supervisor over the Syms Operating Theatre.
The Syms Theatre, opened in 1892, was one of the most advanced operating theaters in the country and had very high standards. Medical students from the College of Physicians and Surgeons, located across the street from the Hospital, trained there, and visiting surgeons frequently came to observe surgical procedures in its sky-lighted amphitheater. As Nurse Supervisor, Galloway had to make sure all her student nurses knew how to properly sterilize instruments, suture materials, towels, and sheets for surgery, something that was a long and complex process at that time, as well as how to work with the surgeons during a procedure. Galloway, noted as being a patient and kind teacher, earned the nickname, “Mother Galloway,” used by students and doctors alike.
Her Hospital service was interrupted only twice in her career – the first time was in 1915, for six months, while Galloway volunteered to work in France with the American Ambulance Corps, prior to the formal U.S. entry into World War I. When the U.S. joined the conflict, Galloway served as a member of Base Hospital 15, which was composed of doctors, nurses, and support staff all drawn from Roosevelt Hospital’s personnel. She served as the Nursing Supervisor, organizing the operating room staff much as she did in the Syms Theatre.

Officers and Nurses of Base Hospital 15. Elise Galloway is on the left, standing next to the Unit Head wearing the Mountie-type hat.
The unit remained in Chaumont, France for most of the war. However, Galloway, along with another nurse and, two doctors spent about ten weeks at a French evacuation hospital at the French front near Vasney, where she experienced air raids at close range in exchange for valuable experience in wound treatment techniques.
Returning home to the Syms Theatre and New York, doctors knew her as an invaluable assistant and friend; nurses knew her as an excellent teacher. She was said to have an unfailing good temper, always calm, retaining poise in any emergency, and very unselfish, presenting the profession of nursing nobly and exemplifying the spirit of service and high standards that nursing is strives for.
The alumni newsletter notes that Elise Galloway left Roosevelt Hospital after an operation in the summer of 1933, and died in the Hospital on September 20, 1934 after an illness of several months.
Dec 7, 2020
The Emergency Medical Service (EMS) has its roots in battlefield medical care, dating back as far as ancient Greece. American emergency medical services began to take the form we recognize today during the Civil War, when plans for medical care of battlefield injuries was organized in an intentional fashion under General George B. McClellan.
The first American civilian ambulance corps formed in Cincinnati, Ohio in 1865. New York City soon followed with its first ambulance service at Bellevue and Allied Hospital, a public hospital, in 1869, under the direction of the newly appointed NYC Sanitary Superintendent, Edward Dalton, MD, a former Union Army surgeon. Private hospitals soon followed suit.
It was common when Roosevelt Hospital opened in 1871 for patients to arrive by themselves, if mobile, or to come in aided by family or friends. However, Hospital Superintendent Horatio Paine, MD, was worried and informed the Board of Trustees that
…persons injured accidentally or overcome by heat in the immediate neighborhood of the Hospital are carried by the police almost invariably, first to the police station in 47th street, and thence by ambulance, … to the Reception Hospital in 99th street … a distance of over 2 and a half miles. Persons injured or sun-struck on the very block on which this Hospital stands, have thus been carried past its doors.
Dr. Paine feared that Roosevelt Hospital would incorrectly appear as unwilling to receive or care for emergency cases at any hour. He collaborated with other hospitals and City authorities to establish ‘casualty districts’ in the City, and in September of 1877, Roosevelt Hospital established an ambulance service for emergency care and, along with St. Luke’s, New York, and Bellevue Hospitals, provided coverage over one of the casualty districts mapped out by the City.
 Horse-drawn carts were the norm from the start of Roosevelt’s service until 1900. Equipment for each of the two ambulance carts may have included tourniquets, sponges, bandages, splints, blankets, and if called for, a straitjacket. This kit was stored under the driver’s seat, along with a quart of whiskey or brandy, which was used as pain relief at that time. At first, the ambulance deployed with only a driver, but it soon became clear that an on-board physician to assess a patient’s condition and perhaps administer treatment while on route to the hospital was necessary. House staff were the first assigned to this service, in rotation. Later on a team of ‘ambulance surgeons’ was formed as a regular unit under the surgical service.
Horse-drawn carts were the norm from the start of Roosevelt’s service until 1900. Equipment for each of the two ambulance carts may have included tourniquets, sponges, bandages, splints, blankets, and if called for, a straitjacket. This kit was stored under the driver’s seat, along with a quart of whiskey or brandy, which was used as pain relief at that time. At first, the ambulance deployed with only a driver, but it soon became clear that an on-board physician to assess a patient’s condition and perhaps administer treatment while on route to the hospital was necessary. House staff were the first assigned to this service, in rotation. Later on a team of ‘ambulance surgeons’ was formed as a regular unit under the surgical service.
Ambulance service gained acceptance over time, as hospitals began to be seen as a safe place to go, a place for healing. For the year 1883, the hospital answered over 734 calls and spent $1,714.11 on feed, straw, repairs, harnesses, horseshoeing, telegraph service, purchase of horses, and also for legal expenses for accidents. That year the service also spent $1,310.92 on whiskey, wine, ale, porter, beer, and mineral waters! By its tenth year of service, ambulance calls rose to 1,122. By its twentieth year of service in 1897, total calls more than doubled the number at 3,300.
The Hospital annual report for 1899 notes that a new accident building opened with a ground floor emergency room and an ambulance court, placing more emphasis on emergency services overall. Accordingly, the service expanded to three ambulances and drivers, answering 4,041 calls.
By 1900 the horse-drawn ambulance was replaced by electric cars, which weigh 4,800 pounds and traveled at up to sixteen miles an hour. Costing $3,000.00 each, the Hospital received two as gifts – one of which was from a prominent physician of the city. The vehicles were seven feet, six inches long on the inside, eighteen inches longer than most ambulances, and had room for three reclining patients, or eight patients if they sat up. The cars were battery powered. The batteries were in a box suspended from the body of the vehicle, to be recharged each time the car returned to the Hospital. In an emergency, an extra set of batteries came with the car and could be put into place in two minutes. The batteries ran 25 miles on one charge.
Service costs ran between $3,000 and $4,000 for each vehicle in 1901 and 1902, in addition to the cost of re-fitting the necessary mechanical arrangements to store them in the old horse stables on the hospital grounds. Costs to run the service rose to $6,000 in 1903, when Hospital administrators decided to discontinue the electric cars, and return to the cheaper and more dependable horse-drawn carts.
On March 1, 1909 the ambulance service was completely discontinued, again, citing the high operational costs, partly due to the legal costs of frequent accidents. New York, Flower, and J. Hood Wright Hospitals stepped in to cover the area left without service.
That same year the State Charities Aid Association published a bill to create a Board of Ambulances – a central control agency over ambulance service in the City. Called The Newcomb-Hoey Bill, it suggested that such a Board consist of the Commissioner of Police, the Commissioner of Public Charities, and the President of the Trustees of Bellevue and Allied Hospitals. Such a Board would cover service over Manhattan and the Bronx. A sister agency, run by the Commissioner of Public Charities, would have control over Queens, Brooklyn, and Staten Island.
Each Board would have general control over and establish the rules and regulations governing all ambulance service in their districts, except those maintained by the Board of Health. It would establish casualty districts, and be the central clearinghouse to receive and distribute ambulance calls to the various hospital units.
The late 1930s was a time of self-assessment and re-evaluation for Roosevelt Hospital. The Hospital was nearly 70 years old and the facilities needed renovation, updating, and expansion to meet the growth of the neighborhood it served. Part of this renewal was the reintroduction of the ambulance service.
On July 5, 1939, at noon, Roosevelt Hospital resumed its ambulance service with modern motor vehicles. Two new ambulances, painted dark gray and white, cost $3,000 each. The Department of Hospitals and the Hospital shared the cost of the service’s operation. Ambulance drivers received extensive training in first aid, especially in dealing with fractures, because World War I had depleted the medical staff and a physician couldn’t be spared. The 1939 Hospital annual report lists five doctors appointed as ambulance surgeons, but they did not ride with the car unless requested by the police officer calling for it.
Prior to its discontinuation in 1909, Roosevelt Hospital’s ambulance answered calls from West 27th Street to West 86st Street and from the Hudson River to Sixth Avenue, including Central Park below 86th Street. When the service resumed in July of 1939, its area covered West 39th to West 72nd Streets between Fifth Avenue and the Hudson, including all of Central Park south of 86th Street.
In the mid-1940s the eastern border of its service was moved to the west side of Park Avenue, except for the area around Grand Central Station, which was served by Grand Central Hospital, and then again to the west side of Lexington Avenue. At this point, Roosevelt Hospital covered the largest casualty district in the City.
Emergency Department renovations in 1961, along with the closing of Grand Central Hospital that same year, forced the expansion of the ambulance district by 130 additional city blocks. The Hospital now covered midtown Manhattan from the Hudson to the East River between East 42nd Street and East 79th Street. Lenox Hill Hospital resumed its ambulance service in 1965, allowing Roosevelt Hospital to reduce its northern border from East 79th Street to East 59th Street and its eastern border returned to the west side of Fifth Avenue.
By 1946 World War II was over and New York City’s population was growing again. The ambulance service was in high demand with 9,166 calls for the year, causing the Hospital to add two additional ambulance cars to the service. The increase in demand put stress on the Accident Ward facilities, which opened in 1899. The following year, demand was even higher with 10,685 calls and 39,329 emergency cases.
In 1947 friends of Dr. James I. Russell, a beloved and distinguished Roosevelt surgeon who had died in 1944, together with other friends of the Hospital, raised funds to construct a building to house modern accident and emergency facilities and a new surgical ward. Named the James I. Russell Memorial Building, the building featured a new, enlarged ambulance bay off 9th Avenue. The first floor handled emergency cases and the second floor was devoted to operating and treatment rooms for 46 surgical patients, and included X-Ray facilities, a plaster room, and eight observation rooms. The Hospital broke ground for the new building in August of 1948 and it opened in June of 1949.
The 1950s saw a continued expansion of the ambulance service and the upgrading and specializing of ambulance car models. In September 1956, three ambulances of a new design, made especially for metropolitan service by the Hospital Ambulance and Purchasing Department personnel, went into service. Their uniquely designed square bodies afforded room to carry four patients on stretchers, in double-decker fashion, or eight persons seated. Peter B. Terenzio, President and Director of the Hospital said the new design provided a ”functionally safe mobile unit which will permit more efficient patient care.” The new two-tone light gray ambulances were the gift of the J.P. Stevens Company, a textile concern, and the Theodore Luce Foundation.
In 1968 the Chief of Ambulance Services designed a new ambulance, for the Hospital. This ambulance, paid for with funds raised by the Hospital’s volunteer corps through the Generosity Thrift Shop, contained many life-saving devices, including an apparatus that provides vital anti-shock treatment while the vehicle is enroute from accident to Hospital.
By the 1960s automobiles were the standard mode of transportation, utilizing a growing system of roadways around the city as well as across the country. The increase in traffic provided an additional challenge to public health and safety. This problem was brought to national attention when President John F. Kennedy noted that, “Traffic accidents constitute one of the greatest, perhaps the greatest, of the nation’s public health problems.” In 1966, President Lyndon B. Johnson declared that traffic accidents were, “…the neglected disease of modern society.”
In 1970 the National Highway Traffic Safety Act was adopted. Amongst several things, the Act standardized EMS training and urged the adoption of a single emergency number countrywide. Use of the 911 emergency number began in 1968, but was slow in gaining acceptance by every state. In 1973 the Federal EMS Systems Act was established, forming 300 EMS systems across the country, including NYC EMS, and the beginning of sweeping changes in EMS care and development across the country.
In the 1970s to 1990s, NYC’s EMS operated under the New York City Health and Hospitals Corporation, which dispatched both its own ambulances and hospital-owned ambulances. On March 17, 1996, NYC EMS merged with the Fire Department of New York (FDNY), forming the Bureau of Emergency Medical Services. FDNY EMS now controls the operation of all ambulances in the NYC 911 system, 70% of which are FDNY-based and 30% hospital-based, supplemented by private ambulance services.
Nov 24, 2020
Whenever you look back to the past, it is easy to find it all very strange, but a longer look allows us to see the threads that connect that time to this. Some of those threads are strong and enduring and others fray and end.
One of those strong threads that tie the Mount Sinai of 100 years ago to the Mount Sinai of 2020 is research and discovery. In 1920, Mount Sinai was dealing with the last wave of a deadly worldwide pandemic that had started in 1918 but still lingered. Some Mount Sinai physicians spent a great deal of time working on a “peculiar disease” that followed the epidemic. This was popularly called the ‘sleeping sickness,’ but doctors termed it epidemic encephalitis. Another Mount Sinai physician was lending his expertise as a member of a national commission that was established to deal with the ravages of empyema, which too often followed post-influenzal pneumonia. Other physicians were doing research on gastric diseases, leukemia, surgical innovations and cardiac problems – all topics that Sinai doctors continue to pursue.

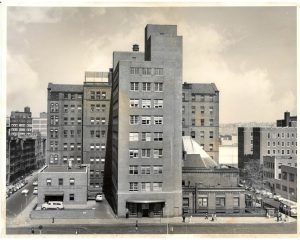
Taken from 5th Ave. and 99th St. looking east over the new buildings. The building facing with the flag pole is the 1904 main building.
Another main theme from 100 years ago, as in every decade of Mount Sinai’s existence, was the physical changes being made on campus. The world war and epidemic had delayed the progress of the largest expansion plan ever envisioned by The Mount Sinai Hospital. First suggested in 1913, it was only in 1922 that all of the new buildings were completed and the renovations of older spaces finished. This resulted in a new Private Pavilion (our current Kravis Children’s Hospital), a new pediatric pavilion and pediatric clinic building, a larger employee dormitory, a larger laboratory building, and a new auditorium to accommodate Mount Sinai’s increasing educational efforts. The growth in the number of beds called for a larger house staff than before and allowed for the growth of new specialty services.
W hile these themes have echoes with our current year, as does the perennial nursing shortage of that era (among many others), there was much that was unique to Mount Sinai in 1920. In February of that year, Mount Sinai leaders held an event to celebrate the staff that had served in the World War I Mount Sinai affiliated unit, Base Hospital No. 3. Special commemorative medals were given to each veteran.
hile these themes have echoes with our current year, as does the perennial nursing shortage of that era (among many others), there was much that was unique to Mount Sinai in 1920. In February of that year, Mount Sinai leaders held an event to celebrate the staff that had served in the World War I Mount Sinai affiliated unit, Base Hospital No. 3. Special commemorative medals were given to each veteran.
The other topic of great interest in 1920 was the re-structuring of the medical staff to combine the in-patient and out-patient services under the in-patient chief of service. The Dispensary and the ward service had been two separate entities with limited overlap. The change allowed the clinic physicians to follow their patients when admitted to the hospital wards, and the ability to round and work with the in-patient staff made it more appealing to community physicians to take on clinic work. In the 1920 Annual Report, it was noted that the combined medical staff now numbered 250 physicians.
Certainly, times change. Institutions changes. Medicine changes. But even 100 years later, at Mount Sinai, some things never change.